





The 1,000-year Legacy of Ibn Sina, Dr. Roy Casagranda & Museum of the Future’s Lessons from the Past
by Media Desk


Infectious diseases have been the subject of much interest in the history of medicine. Significant concepts such as the development of germ and miasma theories have been widely studied and interpreted for diverse audiences. However, historic Muslim contributions to the field of medicine have received less attention. Here, we use the cases of leprosy, the Black Death and smallpox to explore the varied understandings of, and responses to, infectious diseases throughout the Muslim Civilisation (c.7-14th CE). This is a lay introduction to the ways that diverse Muslim societies have approached infectious diseases, and how this has been impacted by religion, in addition to differing social and historical contexts.

Article Image banner by Jemo (©MidJourney CC BY-NC 4.0)
***
Note: This article was written – by Megan Bridgeland, University of Manchester (MSc History of Science, Technology and Medicine student) – as part of a University of Manchester placement with the Foundation for Science, Technology and Civilisation, focusing on the 1001 Cures timeline. The article, therefore, relies heavily on papers published on muslimheritage.com and on two books produced by the Foundation[1].
***
Throughout history, infectious diseases have been an ever-present companion to human existence. Major outbreaks have claimed millions of lives and left a lasting impact on populations, politics and economies. The Muslim Civilisation, which flourished for several hundred years (c.7th-14th CE) and stretched from Spain to parts of China, was no stranger to infectious disease. Some describe Muslim responses to epidemics within this period as uniform and pessimistic[2]. Unsurprisingly across such a vast expanse of time and space, this was not the case. Scholars, physicians and lay citizens within the Muslim World had complex and diverse ways of understanding and reacting to illness. This article takes a look at the varied responses to some of humankind’s most ancient and devastating diseases.
Today, we use the germ theory to understand infections[3]. Developed throughout the 19th century, the germ theory states that infectious diseases are caused by microorganisms (germs) invading the body (see Fig. 1). Over the many centuries before this became widely accepted however, there were various other ways of explaining the sources of disease.

Figure 1. In this satirical 19th-century image, a woman drops her teacup in horror when she sees all of the microscopic organisms that live in the Thames water. ( Source CC-BY-4.0 wellcome.org no. 12079i) – Archived
In early accounts from the Muslim Civilisation, certain epidemics were thought to be a punishment from God. The bubonic plague of ‘Amwas, which struck invading Muslim armies in Syria (c.638) was believed to be punishment for the actions of earlier populations[4]. However, in an act of divine mercy, Muslims who died from this plague were said to become martyrs[5].
Many of the accounts of the plague of ‘Amwas were collected within Ḥadīth (collections of prophetic traditions). In Islam, Ḥadīth are records of the sayings and guidance of Prophet Muhummad (d.632), which were recorded and passed on by chains of narrators. One of these sayings was:
“If you hear of an outbreak of plague in a land, do not enter it; but if the plague breaks out in a place while you are in it, do not leave that place.“ [6]
Today, this guidance sounds very similar to our modern concept of quarantine (or isolation, if we think of COVID-19 responses).
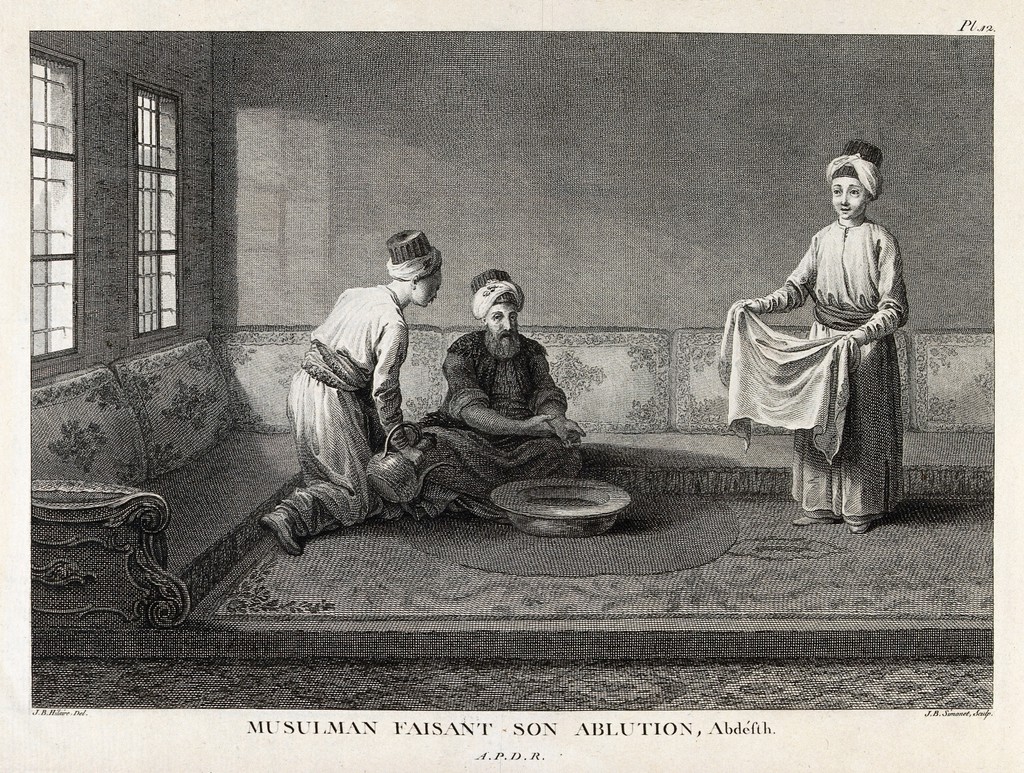
Figure 2. A Muslim man performs Wuḍūʾ, the ritual of washing before prayer (c.1753-1822). Two servants attend to him (Source CC-BY-4.0 wellcome.org no. 33886i) – Archived
Due to the Prophet’s unique status in Islam, Ḥadīth are considered highly important in religious law and guidance, second only to the Qur’an. The Qur’an is a book containing verses recited by the Prophet as words of God (Allah). The Ḥadīth are collections of sayings and descriptions of the Prophet’s life, as narrated by his companions. It is important to note that the Ḥadīth chroniclers classified the narrations into categories according to the strength of their authenticity and the personalities along the chain of narrators. The main classifications include: Sahih (Correct), Hasin (Good), Zaeef (Weak) and Mawdhuo’ (False). Prophetic traditions have been influential within the field of medicine and healthcare.
“Cleanliness is half of faith”[7]
This saying illustrates the significance of good hygiene in Islam. The importance of cleanliness, both physically and spiritually, for Muslims is demonstrated by the paired practices of washing and praying 5 times a day (see Fig. 2).
Several other Ḥadīth are also related to preventative medical practices. These include eating a balanced diet and keeping sources of drinking water separate from toilet waste[8]. Today, framed by the germ theory, we can understand how many of these long-held traditions were important in helping to prevent the spread of infectious diseases.

Figure 3. A depiction of the 4 humoural temperaments (clockwise from top left: phlegmatic (phlegm), sanguine (blood), choleric (yellow bile) and melancholic (black bile). Each temperament is also linked to signs of the zodiac and the 4 elements (c.1574) (Source) – Archived / Public Image – Archived
In the 9th century, due to a significant translation movement, the miasma theory of infectious diseases became dominant in Muslim Civilisation[9]. This theory explained diseases as being caused by poisonous and putrid vapours, or miasmata. Miasma theory dates back to the Classical Greek period (5th-4th BCE), and was advanced by Hippocrates. Hippocrates, often titled the Father of Medicine, believed that 4 bodily fluids (black bile, yellow bile, phlegm and blood) were responsible for the makeup of each individual’s unique characteristics, temperament and health (see Fig. 3). If the balance of these humours was disturbed, this could result in illness or death. Once inhaled, miasmata were believed to disrupt the humours and make the individual ill[10].

Figure 4. Scholars meeting at a library in Baghdad, c.1237 Did you know? For 500 years Baghdad was the thriving capital of the Muslim Civilisation. The city was home to the House of Wisdom (built c.786-809), a huge intellectual academy where scholars from across the globe met to research, debate and collect the world’s knowledge. Find out more here: ©1001inventions.com – Archived
In 9th century Baghdad, scholars from diverse backgrounds translated a vast quantity of medical work from former Greek, Indian and Persian civilisations (see Fig. 4). From this, and from the remnants of Babylonian and Sumerian traditions, they adopted and developed several ideas, including humoural theory. Many influential scholars and physicians, both during and after this period (for example, al-Ṭabarī, al-Rāzī and Ibn Sīnā) drew on this work. As a result, they considered certain diseases, such as leprosy and plague, to be contagious. However, using miasma theory, they believed that these diseases were transmitted through corrupted air, rather than the transfer of microorganisms (which is our understanding of contagion today)[11].
Leprosy was a highly feared disease throughout the Middle Ages, and patients were often shunned by society. The dominant Christian belief in medieval Europe (specifically 11th-14th CE) was that leprosy was a punishment from God for sinning. Sufferers were given bells and special clothing to warn others as they approached — outside of their homes or special hospices they were feared and ostracised (see Fig. 5)[12].

Figure 5. 15th century English depiction of someone with leprosy. The illustration shows the bell that lepers were made to carry in Europe (Source) CC0 1.0 Universal British Library – Archived
Very early on in the Muslim World, however, lepers were separated from others, but cared for and treated humanely. What is often regarded as the first recorded hospital (bīmāristān) in the Islamic World, built by Caliph Walīd ibn ʿAbd al-Malik in 707 CE, was a leprosarium. Slightly later bīmāristāns included separate leprosy wards. Patients were treated by specialist physicians and given regular provisions, rather than being outcasts (see Fig. 6)[13].

Figure 6. Entrance of Sultan Qalawun’s complex in Cairo, Egypt (built 1285), with ablaq decoration. (Source) – Archived CC BY 3.0 by Sailko
Did you know? Hospitals in medieval Islamic civilisations were called Bimaristans. Bimaristans were incredibly well-organised institutions, often providing multiple specialised mental and physical healthcare services, as well as medical education. They were very similar to today’s hospitals!
The al-Mansur Qalawun Complex in Cairo, which dates back to c.1284-5. The complex included a bimaristan. A policy statement from its opening declares that there is no cost for treatment:
“whether the people come from afar or near, whether they are residents or foreigners, strong or weak, low or high, rich or poor, employed or unemployed, blind or signed, physically or mentally ill, learned or illiterate […] there are no conditions of consideration and payment; none is objected to or even indirectly hinted at for non-payment. The entire service is through the magnificence of God, the generous one”[14].
“Flee from a leper as you flee from a lion”[15]
To the non-expert in Ḥadīth classification, the sayings sometimes appear contradictory. This is due to a lack of distinction between the Ḥadīth categories. For example, the Prophet advised to flee from lepers and he refused to accept the oath of allegiance of a leper in person[16]. However it was also reported, in a weak narration, that he invited someone with leprosy to eat from the same bowl as him[17].
All Muslim physicians would have been familiar with religious studies, as they would have learnt to read and write using the Qur’an. However, the ways in which different scholars have interpreted and understood both religion and science are complex and multifaceted. Due to disagreements on the classifications or veracity of Ḥadīth, prophetic traditions have not universally been accepted by Muslim scholars across time, and many theological debates have arisen. For instance in the 9th century, the Mu’talizah questioned the Ḥadīth, using examples to demonstrate that many sayings were contradictory (see Fig. 7). This school of thought was sceptical of the growing list of supposed prophetic traditions, and emphasised the importance of human reason[18]. Others defended the Ḥadīth, arguing that they were in fact logical and compatible with observation, so long as they were read and understood within their individual contexts (this side emerged as the more influential view within Sunni Muslim scholarship)[19].
Figure 7. An image of Socrates painted by Arabs during the Middle Ages. Well over a century old (Source) – Archived. The Mu’taliza (“Withdrawers”) were a group of 9th Century rationalist scholars who promoted human reason over religious scripture (Source) – Archived
This shows us how religious literature can be interpreted in various ways. Often faith and science are assumed to be at odds with each other, but this is not always the case. In these debates, different groups of Muslim scholars used examples from the Ḥadīth and the Quran to argue both for and against the compatibility of religion and scientific values.
The Black Death was a bubonic plague pandemic which devastated Asia, Europe and North Africa in the mid-14th century (see Fig. 8). The plague, which recurred several times over the subsequent decades, had a fatality rate of around 30-60%[20].

Figure 8. The mass burial of plague victims in Belgium, 14th Century (Source) – Archived / (Public Image) – Archived
Following prophetic guidance to not flee the plague, the Andalusian physician and scholar Ibn Khātima al-Anṣārī (1299-1369) remained in his city of Almeria when an outbreak of the Black Death occurred. He treated patients while observing and recording the epidemic[21].
Al-Anṣārī documented all of his observations in a book entitled Taḥṣīl Gharaḍ al-Qāṣidfī Tafṣīl al-Maraḍ al-Wāfid (The Fulfilment of the Inquirer’s Aim Concerning All About the Invading Epidemic). He followed miasma theory, believing that the plague was spread through putrid vapours emitted from severely ill and dying patients (see Fig. 9)[22].

Figure 9. A Turkish funeral, c.1553 – Public Image – Archived
To explain this, he used evidence from Almeria’s Second Hand Shop Market. This market was where the bedding and clothes of the dead patients were taken to be sold. Most of the shopkeepers at this market died from the plague, in contrast with other markets where the death rate was lower, in line with the rest of the population. Al-Anṣārī attributed this to the shopkeepers inhaling vapours absorbed by the bedding that the patients had used while they were ill. He also noted that castles and other secure areas were protected from the plague until a sufferer came into close contact with the household[23].
Al-Anṣārī’s writings show us how observation and empirical evidence have been used throughout time to support different theories of disease. Of course today, these findings are probably explained by infected fleas being carried on the clothes and bedding sold at the markets, and by those visiting the castles.
Constant recurrences of the plague led to many treatises being written by Muslim scholars in this era. Diverse opinions and topics were demonstrated across these writings. As we have seen above, Al-Anṣārī focused on the contagiousness of the Black Death. Others, such as al-Lakhmī (b. 1327) authored public health guides focused on preventing the spread of the disease[24]. At a similar time further East, however, scholars such as Ibn al-Wardī (d. 1349) and al-Manbijī (d. 1383), disputed theories of contagion and argued that the plague was a divine punishment, which could result in martyrdom[25]. Other authors — particularly those practising Tasawwuf (Sufism) — focused on promoting the moral duty of Muslims to stay at an outbreak and care for the sick (see Fig 10)[26].
Figure 10. An 1883 illustration, depicting renowned Muslim physician, al-Zahrāwī (c.936-1013) treating a patient at a hospital in al-Andalus (Muslim Spain). – Archived
There were many more medico-religious debates around the 13th/14th Century. For example, on the topic of disease transmission, some scholars argued that diseases had their own nature (given by God) and could therefore transmit themselves between humans. The more dominant school of thought however, was that diseases did not have their own agency and, as with all Creation, were entirely dependent on the will of God. To complicate this further, those who believed that diseases were completely reliant on God could still support theories of contagion. In this case, God was believed to create unique, coinciding events that allowed for disease transmission[27].

Figure 11. The Jannat al-asmā (“Garden of Names”): an anti-plague talisman (c. late-18th Century). The letters and numbers within the circular motif represent verses from the Qur’an and ʾasmāʾu llāhi l-ḥusnā (Allah’s Beautiful Names). To activate the powers of the talisman, the owner is invited to carry and gaze at the “noble circle” everyday, especially if they are ill. Other texts recommend kissing or rubbing the talisman: wear at the gold centre of the circle suggests that this talisman might have been used in such a way (Topkapı Palace Library, Istanbul, E.H. 1005, folios 20v-21r. Photo by Christiane Gruber) – Archived
As we can see, religious literature was interpreted in diverse and complex ways throughout the Muslim World to support a variety of ideas about infectious diseases and science. Furthermore, religious concepts were also often combined with medical and superstitious beliefs, remedies and objects in the treatment and prevention of disease. These included diet, bloodletting, herbal concoctions, magic, amulets and talismans[28].
Plague was the subject for many treatises. However, one disease that received surprisingly little scholarly attention for several centuries was smallpox. Smallpox was an ancient disease that killed 1 in 3 of those that it infected. Highly contagious, smallpox was characterised by fever, vomiting and blistered skin ‘pustules’ (pox). The disease spread across the world via trade routes and devastated many populations, until it was eradicated by vaccination in 1979[29].
Despite its continuous prevalence and distinctive characteristics, very little was written about smallpox for hundreds of years. That was, until the renowned Muslim physician Abu Bakr Muhammad ibn Zakariya al-Rāzī (d. 925) (or Rhazes, in Latin), wrote his influential text Kitab fi al-Jadari wa-‘l-Hasaba (A Treatise on Smallpox and Measles) (see Fig.12)[30].
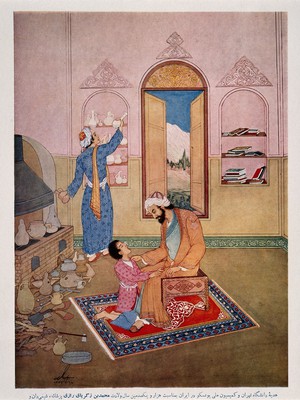
Figure 12. A 20th-century painting of the Persian doctor, al-Rāzī. He is examining a patient, preparing for surgery. (Source CC-BY-4.0 wellcome.org no. 21257i) – Archived
Unable to find a satisfactory text already written on the subject, al-Rāzī was the first to detail the specific differences between smallpox and measles; before this, the two diseases were regarded as the same. Today this is called a differential diagnosis. For example, he wrote that, though fever and breathing difficulties are common in both diseases, back pain is more prominent in smallpox, while anxiety and distress are more common in measles. The book also explored the transmission, treatment, management and prognosis of smallpox[31].
This treatise was extremely important. It was reprinted for over 1000 years in many languages[32]. The work also clearly influenced several physicians born after al-Rāzī (for instance Ibn–Sīnā, one of the most influential scholars of the Islamic Golden Age)[33].
One of al-Rāzī’s observations was that those who survived smallpox did not suffer from the disease again: this is the foundation for vaccination. Before the smallpox vaccine was discovered, however, a practice known as variolation was used to protect against the deadly illness.

Figure 13. Lady Mary Wortley Montagu in Turkish dress, c.1717. – Public Image – Archived
Variolation consisted of taking a small amount of pus from a patient with mild symptoms and introducing it into small scratches on the limbs of the person being immunised. This would usually result in a mild form of the disease and, upon recovery, the patient would be immune to smallpox. In some instances, however, the infection could develop into a severe case and become deadly. Furthermore, for a period of time the patient would be a carrier of smallpox and could spread the disease to others who were not immune[34].
“There is a set of old women, who make it their business to perform the operation, every autumn, in the month of September, when the great heat is abated. People send to one another to know if any of their family has a mind to have the small-pox; they make parties for this purpose, and when they are met (commonly fifteen or sixteen together) the old woman comes with a nut-shell full of the matter of the best sort of small-pox, and asks what vein you please to have opened.
She immediately rips open that you offer to her, with a large needle (which gives you no more pain than a common scratch) and puts into the vein as much matter as can lie upon the head of her needle, and after that, binds up the little wound with a hollow bit of shell, and in this manner opens four or five veins“ – Lady Mary Montagu[35]
Variolation was a very old tradition. The first clear reference to the practice was made in China in 1549. It was later employed throughout Africa, Asia, Persia and Turkey. In 1716, Lady Mary Montagu accompanied her husband when he was appointed British Ambassador to Istanbul (see Fig. 13). Here she observed the practice of variolation and, impressed, had both of her children inoculated. She tried to promote the practice to the British medical establishment, but met resistance, both because she was a woman and because it was an ‘Oriental’ practice. However, her efforts eventually paid off and trials began — the procedure became generally accepted in England until 1796[36].

Figure 14. A satirical print (c.1802) depicting the fear and controversy surrounding smallpox vaccination. After receiving “vaccine pock hot from ye cow”, the patients develop large cow-like swellings. Print published June 12, 1802 by H. Humphrey, St. James’s Street. US Library of Congress, Prints & Photographs Division, LC-USZC4-3147. (Source) – Archived
In 1796, building on this practice, physician Edward Jenner recognised that milkmaids who had been infected with cowpox (a disease similar to smallpox, but less serious), never caught smallpox. He then inoculated James Phipps, an 8-year-old boy, with pus from a cowpox pustule — causing a mild illness in the child (see Fig. 14). When James was then challenged with smallpox material he did not become ill[37].
This incredible story demonstrates how thousands of years of knowledge from across the world was brought together to produce the first-ever vaccine. Thanks to this, and an international public health effort led by the World Health Organisation, the ancient and devastating illness was the first — and so far only — human disease to be eradicated globally[38].
A WHO magazine officially announces the worldwide eradication of smallpox 1980 (Source) (Video)
● Plague and Contagion (a chapter from 1001 Cures: Contributions in Medicine and Healthcare from Muslim Civilisation)
● 1001 Cures: Introduction to the History of Islamic Medicine
● A Medical Classic: Al-Razi’s Treatise on Smallpox and Measles
● Lady Montagu and the Introduction of Smallpox Inoculation to England
● Keep your distance – health lessons from the history of pandemics
● Al-Razi on Smallpox and Measles
[1] Pormann, P. (ed.), 1001Cures: Contributions in Medicine and Healthcare from Muslim Civilisation, Manchester:FSTC (2018); Abdel-Halim, R., 1001 Cures: Introduction to the History of Islamic Medicine, Manchester:FSTC (2021)
[2] Stearns, J. ‘Plague and Contagion’ in 1001Cures: Contributions in Medicine and Healthcare from Muslim Civilisation (2018)
[3] Britannica, Germ Theory. Available at: https://www.britannica.com/science/germ-theory [Last accessed: 2/10/22]
[4] Stearns, Op. cit.
[5] Ibid
[6] Al-Bukhari, S., ‘The Collection of Correct Sayings of Prophet Muhammad’, Chapter: “What has been mentioned about the plague”, Book 75, Ḥadīth 43
[7] This Ḥadīth is classified as correct: Muslim, S., The Book of Purification, Book 2, Ḥadīth 1.
[8] Abdel-Halim, Op. cit., p.116
[9] Stearns, Op.cit.
[10] Kannadan, A., ‘History of the Miasma Theory of Disease’, ESSAI, 16(18), (2018), pp.41-3
[11] Stearns, Op. cit.
[12] Hasnain, R., Queijo, J., Laher, S. and Sandahl, C., ‘Islam, Leprosy, and Disability: How Religion, History, Art, and Storytelling Can Yield New Insights and Acceptance’, Societies, 10(6), (2019), doi.org/10.3390/soc10010006
[13] Ibid
[14] Tschanz, D.W. ‘The Islamic Roots of the Modern Hospital’. AramcoWorld, March/April 2017, pp.22-27. Available at: https://www.aramcoworld.com [Last accessed:6/12/2022]
[15] Al-Bukhari, S. Book of Medicine, Book 76, Ḥadīth 27
[16] This Ḥadīth is classified as correct: reported in Muslim, S., The Book of Greetings, Book 39, Ḥadīth 174.
[17] This Ḥadīth is classified as weak: reported in ibn Majah, S., Book of Medicine, Book 31, Ḥadīth 3542.
[18] Stearns, Op. cit.
[19] Ibid
[20] Stearns, Op. cit.; Wade, L., From Black Death to Fatal Flu, Past Pandemics Show Why People on the Margins Suffer Most. Available at: https://www.science.org [Last accessed: 2/10/2022]
[21] Abdel-Halim, Op. cit., pp.119-121
[22] Ibid
[23] Ibid
[24] Ibid, p.121
[25] Stearns, Op. cit.
[26] Ibid
[27] Ibid
[28] Ibid
[29] CDC, History of Smallpox. Available at: https://www.cdc.gov/smallpox/history/history.html [Last accessed: 2/10/21]
[30] Naqvi, N. A Medical Classic: Al-Razi’s Treatise on Smallpox and Measles. Available at: https://muslimheritage.com/al-razis-treatise-on-smallpox/ (2012) [Last accessed: 2/10/2022]
[31] Kaadan, A. Al-Razi on Smallpox and Measles. Available at: https://muslimheritage.com/al-razi-smallpox-measles/ (2007) [Last accessed: 2/10/2022]
[32] Naqvi, Op. cit.
[33] Kaadan, Op. cit.
[34] Zaimeche, S. and Al-Hassani, S. Lady Montagu and the Introduction of Smallpox Inoculation to England. Available at: https://muslimheritage.com/lady-montagu-smallpox-inoculation-england/ (2010) [Last accessed:2/10/2022]
[35] Ibid
[36] Ibid
[37] Ibid
[38] Ibid
Discover the golden
age of Muslim civilisation.
© Copyright FSTC Ltd 2002-2020. All Rights Reserved.









