Wel knew he the olde Esculapius
And Deyscorides and eek Rufus,
Olde Ypocras, Haly and Galeyn,
Serapion, Razi and Avycen,
Averrois, Damascien and Constantyn,
Bernard and Gatesden and Gilbertyn.

Figure 1. Article banner
* * *
Note of the editor
This article was first published in the print edition of Saudi Aramco World (May/June 1997, pp. 20-31) written by David W. Tschanz. We reproduce it with the permission of the publisher. Please also note that – to avoid misunderstanding the title – we believe a better term to use is Arabick instead of Arab, to include all people and nations whose language used Arabic script.
* * *
In the “General Prologue” of The Canterbury Tales , Geoffrey Chaucer identifies the authorities used by his “Doctour of Physic” in the six lines quoted above. The list includes four Arab physicians: Jesu Haly (Ibn ‘Isa), Razi (Al-Razi, or Rhazes), Avycen (Ibn Sina, or Avicenna) and Averrois (Ibn Rushd, or Averroes). These four did not make Chaucer’s list only to add an exotic flavor to his late-14th-century poetry. Chaucer cited them because they were regarded as among the great medical authorities of the ancient world and the European Middle Ages, physicians whose textbooks were used in European medical schools, and would be for centuries to come. First collecting, then translating, then augmenting and finally codifying the classical Greco-Roman heritage that Europe had lost, Arab physicians of the eighth to eleventh century laid the foundations of the institutions and the science of modern medicine.
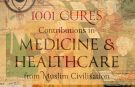
Figure 2. Galen, Ibn Sina (Avecena), and Hippocrates, the three authorities on medical theory and practice in a woodcut from an early 15th-century Latin medical book. (Source).
After the collapse of the western Roman empire in the fifth century, Europe lost touch with much of its intellectual heritage. Of Greek science, all that remained were Pliny’s Encyclopedia and Boethius’s treatises on logic and mathematics; the Latin library was so limited that European theologians found it nearly impossible to expand their knowledge of their own scriptures.
The center of Europe’s new world view became the church, which exerted profound new influences in medicine. Because Christianity emphasized compassion and care for the sick, monastic orders ran fine hospitals—but they did not function as hospitals do today. They were simply places to take seriously ill people, where they were expected to either recover or die as God willed. There were no learned physicians to attend them, only kindly monks who dispensed comfort and the sacraments, but not medicines.
Because the Christian church viewed care of the soul as far more important than care of the body, medical treatment and even physical cleanliness were little valued, and mortification of the flesh was seen as a sign of saintliness. In time, nearly all Europeans came to look upon illness as a condition caused by supernatural forces, which might take the form of diabolical possession. Hence, cures could only be effected by religious means. Every malady had a patron saint to whom prayers were directed by the patient, family, friends and the community. Upper respiratory infections were warded off by a blessing of the throat with crossed candles on the feast of Saint Blaise. Saint Roch became the patron of plague victims. Saint Nicaise was the source of protection against smallpox. Kings, regarded as divinely appointed, were believed to be able to cure scrofula and skin diseases, among other maladies, with the “royal touch.”
 Figure 3. Ibn Rushd in a dialogue with Porphyre in a medieval Latin manuscript Liber de herbis by Monfredo de Monte Imperiali (Source)
Figure 3. Ibn Rushd in a dialogue with Porphyre in a medieval Latin manuscript Liber de herbis by Monfredo de Monte Imperiali (Source)
With the study of disease and of patients neglected, licensed medicine as an independent craft virtually vanished. Those physicians who endured were mostly connected with monasteries and abbeys. But even for them, the generally accepted goal was less to discover causes, or even to heal, than to study the writings of other physicians and comment on their work. In the middle of the seventh century, the Catholic church banned surgery by monks, because it constituted a danger to their souls. Since nearly all of the surgeons of that era were clerics, the decree effectively ended the practice of surgery in Europe.
At roughly the same time, another civilization was rising in the east. The coming of Islam, also in the seventh century (See Aramco World, November/December 1991), led to a hundred years of continuous geographical expansion and an unprecedented era of ferment in all branches of learning. The Arabs rapidly melded the various cultures of the Islamic domain, and Arabic—the language of the Qur’an—became the universal language. By the 10th century a single language linked peoples from the Rann of Kutch to the south of France, and Arabic became to the East what Latin and Greek had been to the West—the language of literature, the arts and sciences, and the common tongue of the educated.
Medicine was the first of the Greek sciences to be studied in depth by Islamic scholars. After Plato’s Academy was closed in 529, some of its scholars found refuge at the university at Jundishahpur, the old Sassanid capital of Persia, which had also sheltered excommunicated Nestorian Christian scholars—among them physicians—in 431. Persia became part of the Islamic world in 636, and Arab rulers supported the medical school at Jundishahpur; for the next 200 years it was the greatest center of medical teaching in the Islamic world. There, Islamic physicians first familiarized themselves with the works of Hippocrates, Galen and other Greek physicians. At the same time, they were also exposed to the medical knowledge of Byzantium, Persia, India and China.
Recognizing the importance of translating Greek works into Arabic to make them more widely available, the Abbasid caliphs Harun al-Rashid (786-809) and his son, al-Ma’mun (813-833) established a translation bureau in Baghdad, the Bayt al-Hikmah, or House of Wisdom, and sent embassies to collect Greek scientific works in the Byzantine Empire. (See Aramco World, May/June 1982.) This ushered in the first era in Islamic medicine, whose effects we feel today: the period of translation and compilation.
 Figure 4. House of Wisdom Sketch © 1001 inventions
Figure 4. House of Wisdom Sketch © 1001 inventions
The most important of the translators was Hunayn ibn Ishaq al-‘Ibadi (809-73), who was reputed to have been paid for his manuscripts by an equal weight of gold. He and his team of translators rendered the entire body of Greek medical texts, including all the works of Galen, Oribasius, Paul of Aegin, Hippocrates and the Materia Medica of Dioscorides, into Arabic by the end of the ninth century. These translations established the foundations of a uniquely Arab medicine.
Muslim medical practice largely accepted Galen’s premise of humors, which held that the human body was made up of the same four elements that comprise the world—earth, air, fire and water. These elements could be mixed in various pro portions, and the differing mixtures gave rise to the different temperaments and “humors.” When the body’s humors were correctly balanceda person was healthy. Sickness was due not to supernatural forces but to humoral imbalance, and such imbalance could be corrected by the doctor’s healing arts
Muslim physicians therefore came to look upon medicine as the science by which the dispositions of thehuman body could be discerned, and to see its goal as the preservation of health and, if health should be lost, assistance in recovering it. They viewed themselves as practitioners of the dual art of healing and the maintenance of health.
Even before the period of translation closed, advances were made in other health-related fields. Harun al-Rashid established the first hospital, in the modern sense of the term, at Baghdad about 805. Within a decade or two, 34 more hospitals had sprung up throughout the Islamic world, and the number grew each year.

Figure 5. Fountains were central to the architecture of the Bimaristan Arghun: Three courtyards each held a fountain, around which patient rooms were arranged, while the central courtryard featured a large rectangular pool and well. (Source)
These hospitals, or bimaristans, bore little resemblance to their European counterparts. The sick saw the bimaristan as a place where they could be treated and perhaps cured by physicians, and the physicians saw the bimaristan as an institution devoted to the promotion of health, the cure of disease and the expansion and dissemination of medical knowledge. Medical schools and libraries were attached to the larger hospitals, and senior physicians taught students, who were in turn expected to apply in the men’s and women’s wards what they had learned in the lecture hall. Hospitals set examinations for their students, and issued diplomas. By the 11th century, there were even traveling clinics, staffed by the hospitals, that brought medical care to those too distant or too sick to come to the hospitals themselves. The bimaristan was, in short, the cradle of Arab medicine and the prototype upon which the modern hospital is based.
Like the hospital, the institution of the pharmacy, too, was an Islamic development. Islam teaches that “God has provided a remedy for every illness,” and that Muslims should search for those remedies and use them with skill and compassion. One of the first pharmacological treatises was composed by Jabir ibn Hayyan (ca. 776), who is considered the father of Arab alchemy. The Arab pharmacopoeia of the time was extensive, and gave descriptions of the geographical origin, physical properties and methods of application of everything found useful in the cure of disease. Arab pharmacists, or saydalani, introduced a large number of new drugs to clinical practice, including senna, camphor, sandalwood, musk, myrrh, cassia, tamarind, nutmeg, cloves, aconite, ambergris and mercury. The saydalani also developed syrups and juleps—the words came from Arabic and Persian, respectively—and pleasant solvents such as rose water and orange-blossom water as means of administering drugs. They were familiar with the anesthetic effects of Indian hemp and henbane, both when taken in liquids and inhaled.
By the time of al-Ma’mun’s caliphate, pharmacy was a profession practiced by highly skilled specialists. Pharmacists were required to pass examinations and be licensed, and were then monitored by the state. At the start of the ninth century, the first private apothecary shops opened in Baghdad. Pharmaceutical preparations were manufactured and distributed commercially, then dispensed by physicians and pharmacists in a variety of forms—ointments, pills, elixirs, confections, tinctures, suppositories and inhalants.
The blossoming of original thought in Arab medicine began as the ninth century drew to a close. The first major work appeared when Abu Bakr Muhammad ibn Zakariya Al-Razi (ca. 841-926) turned his attention to medicine.

Figure 6. In the late ninth century, a leading physician and polymath Muhammad ibn Zakariya al-Razi helped establish a bimaristan—hospital—in Baghdad staffed with 25 doctors, optometrists, surgeons and bonesetters. The illustration above, from a 13th-century European translation of Al-Razi’s Compendium of Medical Treatises, shows him treating a patient. (Source)
Al-Razi, known to the West as Rhazes, was born in Persia in the town of Rayy, near Tehran. After a youth spent as a musician, mathematician and alchemist, Al-Razi went to Baghdad to take up the study of medicine at the age of 40. Completing his studies, he returned to Rayy and assumed the directorship of its hospital. His reputation grew rapidly and within a few years he was selected to be the director of a new hospital to be built in Baghdad. He approached the question of where to put the new facility by hanging pieces of meat in various sections of the city and checking the rate at which they spoiled. He then ordered the hospital built at the site where the meat showed the least putrefaction.
Al-Razi is regarded as Islamic medicine’s greatest clinician and its most original thinker. A prolific writer, he turned out some 237 books, about half of which dealt with medicine. His treatise The Diseases of Children has led some historians to regard him as the father of pediatrics. He was the first to identify hay fever and its cause. His work on kidney stones is still considered a classic. In addition, he was instrumental in the introduction of mercurial ointments to treat scabies. Al-Razi advocated reliance on observation rather than on received authority; he was a strong proponent of experimental medicine and the beneficial use of previously tested medicinal plants and other drugs. A leader in the fight against quacks and charlatans—and author of a book exposing their methods—he called for high professional standards for practitioners. He also insisted on continuing education for already licensed physicians. Al-Razi was the first to emphasize the value of mutual trust and consultation among skilled physicians in the treatment of patients, a rare practice at that time.
Following his term as hospital director in Baghdad, he returned to Rayy where he taught the healing arts in the local hospital, and he continued to write. His first major work was a 10-part treatise entitled Al-Kitab al-Mansuri, so called after the ruler of Rayy, Mansur ibn Ishaq. In it, he discussed such varied subjects as general medical theories and definitions; diet and drugs and their effect on the human body; mother and child care, skin disease, oral hygiene, climatology and the effect of the environment on health; epidemiology and toxicology.
Al-Razi also prepared Al-Judari wa al Hasbah, the first treatise ever written on smallpox and measles. In a masterful demonstration of clinical observation (see column at right), Al-Razi became the first to distinguish the two diseases from each other. At the same time, he provided still-valid guidelines for the sound treatment of both.

Figure 7. “Among Europeans, al-Razi’s most sought after work was his Kitab al-Hawi fi al-tibb (The comprehensive book on medicine), which was translated into Latin in 1279 under the title Continens Rasis by Faraj ben Salim, a physician of Sicilian-Jewish origin employed by Charles of Anjou to translate medical works. This book is also known in Latin as Continens Liber and in English as The Virtuous Life. Shown here is the rare 1529 edition of Continens Rasis, which was printed in Venice by Johannes Hamman” (Source)
His most esteemed work was a medical encyclopedia in 25 books, Al-Kitab al-Hawi, or The Comprehensive Work, the Liber Continens of al-Razi’s later Latin translators. Al-Razi spent a lifetime collecting data for the book, which he intended as a summary of all the medical knowledge of his time, augmented by his own experience and observations. In Al-Hawi, Al-Razi emphasized the need for physicians to pay careful attention to what the patients’ histories told them, rather than merely consulting the authorities of the past. In a series of diagnosed case histories entitled “Illustrative Accounts of Patients,” Al-Razi demonstrated this important tenet. One patient, who lived in a malarial district, suffered from intermittent chills and fever that had been diagnosed as malaria, but nonetheless seemed incurable. Al-Razi was asked to examine him. Upon noting pus in the urine, he diagnosed an infected kidney, and he treated the patient successfully with diuretics.
Al-Razi’s clinical skill was matched by his understanding of human nature, particularly as demonstrated in the attitudes of patients. In a series of short monographs on the doctor-patient relationship, he described principles that are still taught a millennium later: Doctors and patients need to establish a mutual bond of trust, he wrote; positive comments from doctors encourage patients, make them feel better and speed their recovery; and, he warned, changing from one doctor to another wastes patients’ health, wealth and time.
Not long after Al-Razi’s death, Abu ‘Ali al-Husayn ibn ‘Abd Allah ibn Sina (980-1037) was born in Bukhara, in what today is Uzbekistan. Later translators Latinized his name to Avicenna. It is hard to describe Ibn Sina in anything other than superlatives. He was to the Arab world what Aristotle was to Greece, Leonardo da Vinci to the Renaissance and Goethe to Germany. His preeminence embraced not only medicine, but also the fields of philosophy, science, music, poetry and statecraft. His contemporaries called him “the prince of physicians.”
Ibn Sina’s life was in fact the stuff of legend. The son of a tax collector, he was so precocious that he had completely memorized the Qur’an by age 10. Then he studied law, mathematics, physics, and philosophy. Confronted by a difficult problem in Aristotle’s Metaphysics, Ibn Sina re-read the book 40 times in his successful search for a solution. At 16 he turned to the study of medicine, which he said he found “not difficult.” By 18, his fame as a physician was so great that he was summoned to treat the Samanid prince Nuh ibn Mansur. His success with that patient won him access to the Samanid royal library, one of the greatest of Bukhara’s many storehouses of learning.
At 20, Ibn Sina was appointed court physician, and twice served as vizier, to Shams al-Dawlah, the Buyid prince of Hamadan, in western Persia. His remaining years were crowded with adventure and hard work, yet he somehow found time to write 20 books on theology, metaphysics, astronomy, philology and poetry and 20 more on medicine—including Kitab al-Shifa’, or The Book of Healing, a medical and philosophical encyclopedia.
His supreme work, however, is the monumental Al-Qanun fi al-Tibb, The Canon of Medicine. Over one million words long, it was nothing less than a codification of all existing medical knowledge. Summarizing the Hippocratic and Galenic traditions, describing Syro-Arab and Indo-Persian practice and including notes on his own observations, Ibn Sina strove to fit each bit of anatomy, physiology, diagnosis and treatment into its proper niche.

Figure 8. Inside image of the Canon of Medicine book (Source)
The Canon stressed the importance of diet and the influence of climate and environment on health. It included discussions of rabies, hydrocele, breast cancer, tumors, labor and poisons and their treatment. Ibn Sina differentiated meningitis from the meningismus of other acute diseases; and described chronic nephritis, facial paralysis, ulcer of the stomach and the various types of hepatitis and their causes. He also expounded the dilation and contraction of the pupils and their diagnostic value, described the six motor muscles of the eye and discussed the functions of the tear ducts, and he noted the contagious nature of some diseases, which he attributed to “traces” left in the air by a sick person.
The Canon also included a description of some 760 medicinal plants and the drugs that could be derived from them. At the same time Ibn Sina laid out the basic rules of clinical drug trials, principles that are still followed today. (See page 28.)
Not surprisingly, The Canon rapidly became the standard medical reference work of the Islamic world. Nizami-i Arudi of Samarkand spoke for generations of physicians when he wrote, in the early 12th century, “From him who manages the first volume [of The Canon], nothing will be hidden concerning the general theory and principles of medicine.” The Canon was used as a reference, a teaching guide and a medical textbook until well into the 19th century, longer than any other medical work.
During the 10th century, when Arab astronomical texts were first translated in Catalonia, Europe began to reap the intellectual riches of the Arabs and, in so doing, to seek out its own classical heritage. The medical works of Galen and Hippocrates returned to the West by way of the Middle East and North Africa, recovered through Latin translations of what had become the Arab medical classics. Through the intellectual ferment of the Islamic present, Europe recovered some of its past.
The two main translators of classical material from Arabic into Latin were Constantinus (also known as Leo) Africanus (1020-1087), who worked at Salerno and in the cloister of Monte Cassino, and Gerard of Cremona (1140-1187), who worked in Toledo. It was no accident that both translators lived in the Arab-Christian transition zone, where the two cultures fructified each other. And it was no coincidence that Salerno, Europe’s first great medical faculty of the Middle Ages, was close to Arab Sicily, nor that the second, Montpellier, was founded in 1221 in southern France, near the Andalusian border.
Ibn Sina’s Canon made its first appearance in Europe by the end of the 12th century, and its impact was dramatic. Copied and recopied, it quickly became the standard European medical reference work. In the last 30 years of the 15th century, just before the European invention of printing, it was issued in 16 editions; in the century that followed more than 20 further editions were printed. From the 12th to the 17th century, its materia medica was the pharmacopoeia of Europe, and as late as 1537 The Canon was still a required textbook at the University of Vienna.
Translations of Al-Razi’s Al-Kitab al-Hawi and other works followed rapidly. Printed while printing was still in its infancy, all of Al-Razi’s works gained widespread acceptance. The ninth book of Al-Kitab al-Mansuri (“Concerning Diseases from the Head to the Foot”) remained part of the medical curriculum at the University of Tübingen until the end of the 15th century.
Contemporary Europeans regarded Ibn Sina and Al-Razi as the greatest authorities on medical matters, and portraits of both men still adorn the great hall of the School of Medicine at the University of Paris. In The Inferno, Dante placed Ibn Sina side by side with antiquity’s two greatest physicians, Hippocrates and Galen. Roger Bacon consulted Ibn Sina to further his own inquiries into vision.
But it was not only Al-Razi and Ibn Sina who influenced Europe. Translations of more than 400 Arab authors, writing on such varied topics as ophthalmology, surgery, pharmaceuticals, child care and public health, deeply influenced the rebirth of European science.
Despite their belief in now superseded theories such as humors and miasmas, the”medicine of Ibn Sina, Al-Razi and their contemporaries is the basis of much of what we take for granted today.
It was those Arab physicians who made accurate diagnoses of plague, diphtheria, leprosy, rabies, diabetes, gout, cancer and epilepsy. Ibn Sina’s theory of infection by “traces” led to the introduction of quarantine as a means of limiting the spread of infectious diseases. Arab doctors laid down the principles of clinical investigation and drug trials, and they uncovered the secret of sight. They mastered operations for hernia and cataract, filled teeth with gold leaf and prescribed spectacles for defective eyesight. And they passed on rules of health, diet and hygiene that are still largely valid today.
Thus the Islamic world not only provided a slender but ultimately successful line of transmission for the medical knowledge of ancient Greece and the Hellenic world, it also corrected and enormously expanded that knowledge before passing it on to a Europe that had abandoned observation, experimentation and the very concept of earthly progress centuries before. Physicians of different languages and religions had cooperated in building a sturdy structure whose outlines are still visible in the medical practices of our own time.
Figure 9. The miniature depicting of Rustem’s birth by Nursel Uvendire (Original source: Shahnama-i Firdawsī, Turk-Islam Exhibits Museum, Istanbul, MS 1955). Image taken from: Turkish Medical History through Miniature Pictures. ed. Nil Sari, Istanbul 2002.(Source) (Archived)
The Caliphs’ Researches
Fourteenth-century historian and political scientist Ibn Khaldun wrote about the intellectual curiosity that helped to preserve Greek learning.
When the Byzantine emperors conquered Syria, the scientific works of the Greeks were still in existence. Then God brought Islam, and the Muslims won their remarkable victories, conquering the Byzantines as well as all other nations. At first, the Muslims were simple, and did not cultivate learning, but as time went on and the Muslim dynasty flourished, the Muslims developed an urban culture which surpassed that of any other nation.
They began to wish to study the various branches of philosophy, of whose existence they knew from their contact with bishops and priests among their Christian subjects. In any case, man has always had a penchant for intellectual speculation. The caliph al-Mansur therefore sent an embassy to the Byzantine emperor, asking him to send him translations of books on mathematics. The emperor sent him Euclid’s Elements and some works on physics.
Muslim scholars studied these books, and their desire to obtain others was whetted. When al-Ma’mun, who had some scientific knowledge, assumed the caliphate, he wished to do something to further the progress of science. For that purpose, he sent ambassadors and translators to the Byzantine empire, in order to search out works on the Greek sciences and have them translated into Arabic. As a result of these efforts, a great deal of material was gathered and preserved.

Figure 10. The Byzantine embassy of John the Grammarian in 829 to Ma’mun (Source)
In Al-Judari wa al-Hasbah, Al-Razi distinguished smallpox from measles for the first time in medical history. This passage shows his skill as a medical observer, a competence on which he placed great importance.
The eruption of the smallpox is preceded by a continued fever, pain in the back, itching in the nose and terrors in the sleep. These are the more peculiar symptoms of its approach, especially a pain in the back with fever; then also a pricking which the patient feels all over his body; a fullness of the face, which at times comes and goes; an inflamed color, and vehement redness in both cheeks; a redness of both the eyes, heaviness of the whole body; great uneasiness, the symptoms of which are stretching and yawning; a pain in the throat and chest, with slight difficulty in breathing and cough; a dryness of the breath, thick spittle and hoarseness of the voice; pain and heaviness of the head; inquietude, nausea and anxiety; (with this difference that the inquietude, nausea and anxiety are more frequent in the measles than in the smallpox; while on the other hand, the pain in the back is more peculiar to the smallpox than to the measles;) heat of the whole body; an inflamed colon, and shining redness, and especially an intense redness of the gums.
Figure 11. “Lady Montagu and the Introduction of Smallpox Inoculation to England” – The painting Lady Mary Wortley Montagu with her son, Edward Wortley Montagu, and attendants attributed to Jean Baptiste Vanmour (oil on canvas, circa 1717). © National Portrait Gallery, London:NPG 3924.(Source)
Testing New Medicines
In his voluminous writings, Ibn Sina laid out the following rules for testing the effectiveness of a new drug or medication. These principles still form the basis of modern clinical drug trials.
1. The drug must be free from any extraneous accidental quality.
2. It must be used on a simple, not a composite, disease.
3. The drug must be tested with two contrary types of diseases, because sometimes a drug cures one disease by Its essential qualities and another by its accidental ones.
4. The quality of the drug must correspond to the strength of the disease. For example, there are some drugs whose heat is less than the coldness of certain diseases, so that they would have no effect on them.
5. The time of action must be observed, so that essence and accident are not confused.
6. The effect of the drug must be seen to occur constantly or in many cases, for if this did not happen, it was an accidental effect.
7. The experimentation must be done with the human body, for testing a drug on a lion or a horse might not prove anything about its effect on man.
written by David W. Tschanz; read online here.
Discover the golden
age of Muslim civilisation.
© Copyright FSTC Ltd 2002-2020. All Rights Reserved.